1. What is IgE?
In our blood, there exists a special class of protein known as immunoglobulin, which is an important component of the immune system. Among them, IgE (immunoglobulin E), despite its extremely low concentration, accounting for only 0.002% of the total immunoglobulin, it acts as a key "messenger" in triggering allergic reactions. This antibody produced by B lymphocytes primarily protects the human body in two ways: one is to resist parasitic infections, and the other is to trigger an immune response when encountering allergens.
When allergens (such as pollen, dust mites or certain foods) enter the human body, the immune system recognizes them as "foreign invaders" and prompts B cells to produce IgE antibodies against the allergen. These IgE will specifically bind to the surface of mast cells and basophils, causing the body to enter a "sensitized state". When exposed to the same allergen again, IgE immediately activates the "alarm system", prompting cells to release inflammatory mediators such as histamine, triggering allergic symptoms like sneezing, itchy skin, and breathing difficulties - this is the fundamental principle of what we commonly refer to as an allergic reaction.
2. IgE Testing: Purpose and Applications
IgE detection has become a critical tool in the diagnosis of allergic diseases.
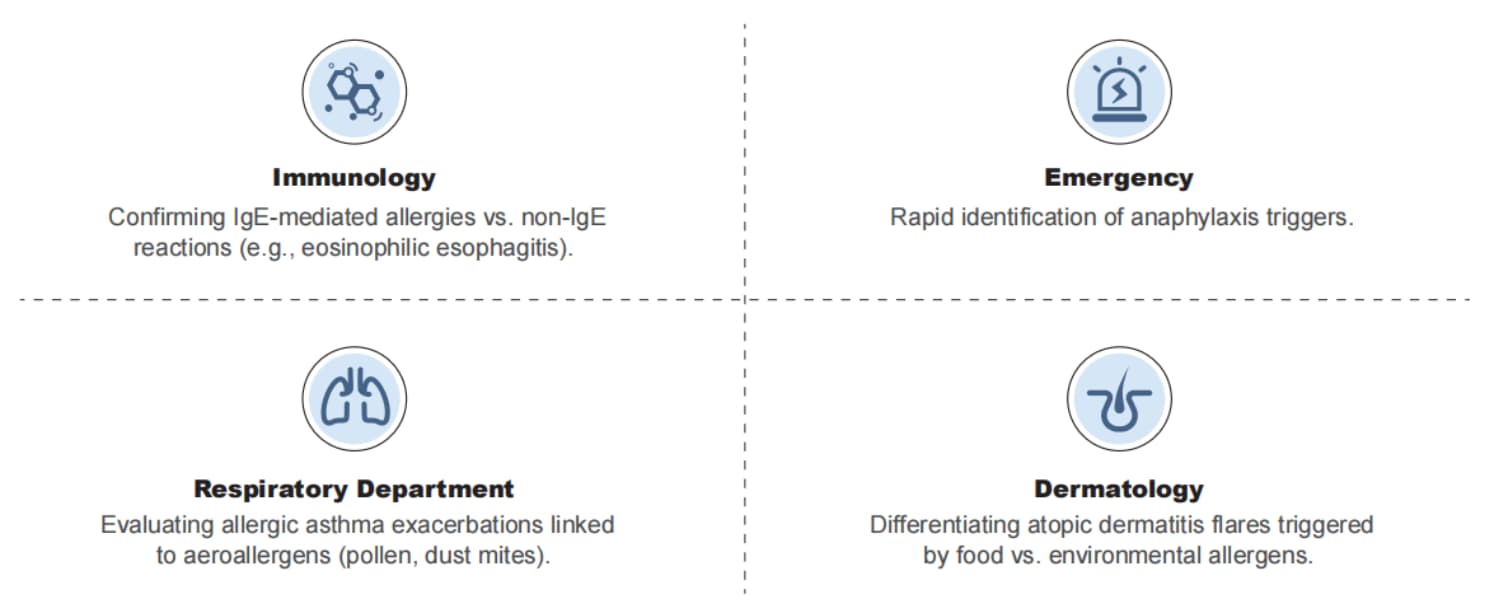
Clinical significance: Studies show that approximately 30% of patients with allergic diseases exhibit significantly elevated levels of total serum IgE. Moreover, specific IgE testing demonstrates over 85% accuracy in identifying the types of allergens involved. This test is mainly applicable to three types of people:
✓ Patients with recurrent skin itching, urticaria, allergic rhinitis and other symptoms.
✓ Individuals with a history of asthma and unknown cause.
✓ High-risk groups with a family history of allergic diseases.
Note: IgE test results must be interpreted in conjunction with clinical symptoms. For instance, in patients with hay fever, allergen-specific IgE levels may rise 2-4 weeks before the pollen season begins. In cases of food allergy, relevant IgE antibodies can trigger an immune response within 1-2 hours after ingestion of the allergenic food. Through dynamic monitoring of IgE levels, physicians can not only confirm a diagnosis but also develop personalized desensitization treatment plans, which have been shown to reduce the risk of acute asthma attacks by 40%-60%.
3. From Testing to Management: Comprehensive Prevention and Control of Allergic Diseases
IgE testing is only the first step in the management of allergic diseases. Clinical practice has shown that personalized prevention and control plans, developed based on test results, can improve patients' quality of life scores by 35%~50%. For patients allergic to dust mites, in addition to the use of antihistamines, regular environmental control measures, such as using mite-proof bedding and air purifiers, can reduce the frequency of symptom episodes by 40%. Patients with food allergies, on the other hand, need to strictly avoid allergenic foods and carry an epinephrine auto-injector at all times in case of accidental exposure.

With advances in precision medicine, IgE testing technology is also continuously evolving. The new generation of testing methods can not only quantitatively analyze antibody levels but also predict the severity of allergic reactions by detecting IgE subtypes.
In an era of ongoing iteration in in vitro diagnostic technologies, Poclight IgE test kit, with its innovative technology, exceptional performance, user-friendly operation, and reliable quality, offers a new option for the precise diagnosis of allergic diseases. In the future, by integrating genetic testing and artificial intelligence algorithms, we hope to achieve early warning and precise intervention for allergic diseases, helping more people break free from the burden of allergies.
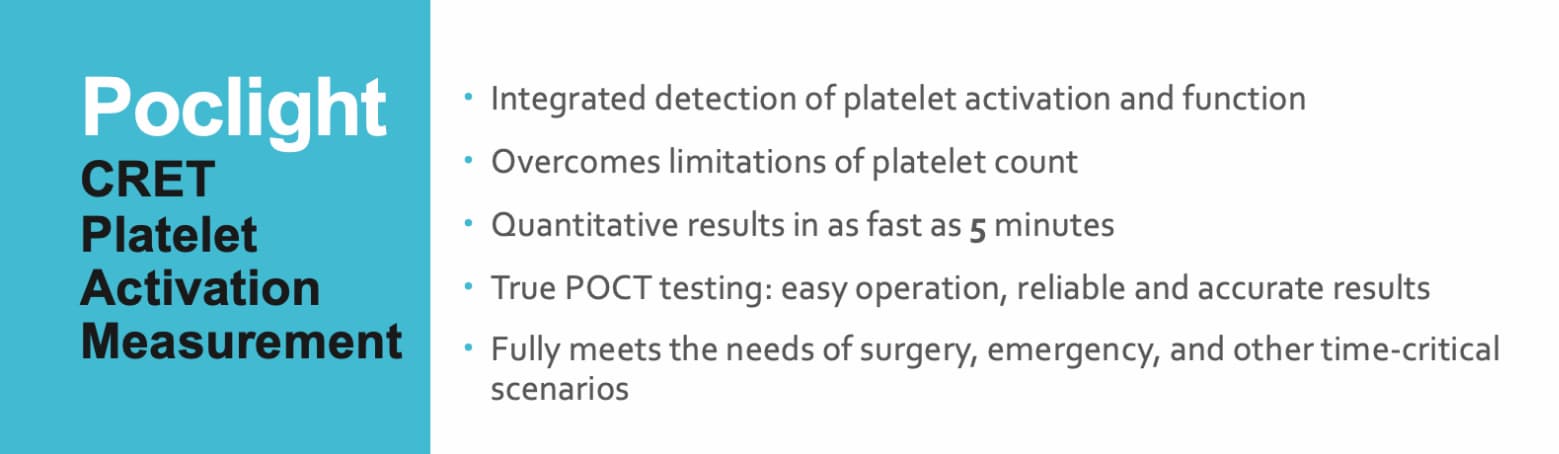
Advantages of Poclight IgE Test Kit: Innovative CRET Technology Enables Precision "Signal-Switch" Detection
Technology Principle:
✓ Utilizes a homogeneous chemiluminescence approach.
✓ Integrates antigen-antibody reactions with chemiluminescent signals.
Workflow:
● The target substance binds with an acridinium ester-labeled DNA antibody to form an immunocomplex.
● Graphene oxide quenches the remaining unbound acridinium ester-labeled DNA fragments.
● This homogeneous process eliminates the need for separation and washing steps.
● A chemiluminescent reaction is initiated by adding an excitation solution.
Performance Specifications:
✓ High Sensitivity: Detection sensitivity of 0.1 IU/mL.
✓ Wide Linear Range: 0.1–2500 IU/mL, fully meeting clinical testing requirements.
✓ Excellent Precision: Intra-assay CV ≤10% and inter-assay CV ≤15%, ensuring stable and reliable results.
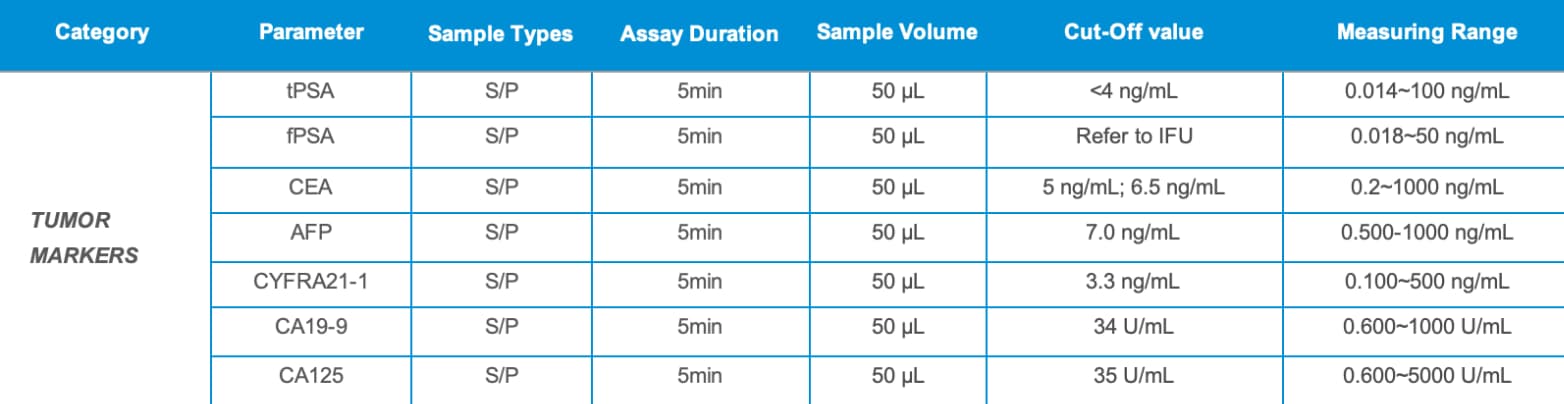
✓ Rapid detection: in just 5 minutes, minimal sample volume of 50 µL, simple operation, low cost, high-quality CLIA methodology, innovative CRET patented technology, precise results, and a wide linear detection range.
✓ Ease of Use: Minimal training required
Key Advantage (vs. Traditional ELISA):
● Exceptional Speed: Reduces the detection time from 3 hours to just 5 minutes.
● Operational Simplicity: The homogeneous assay format removes the need for cumbersome washing and separation steps.
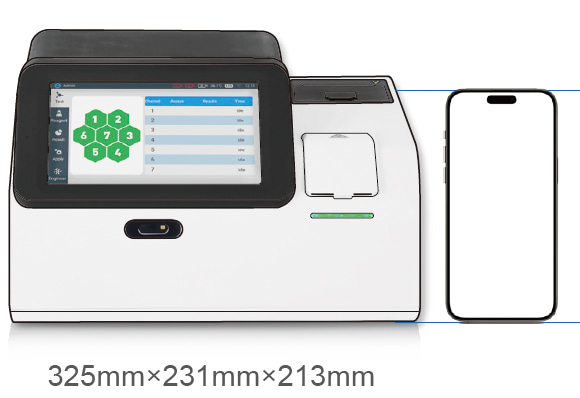
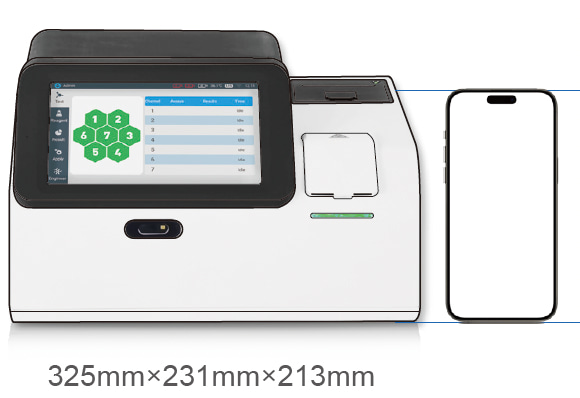
Compatible with Poclight C5000 POC CLIA Analyzer
To learn more about cooperation regarding Poclight's 5-generation CLIA solutions, please contact us.